Hair Miniaturization: What It Means and How to Spot It
Written by the Balding AI Editorial Team · medically reviewed by Dr. Nga Nguyen (Dermatologist) · grounded in published clinical guidelines (AAD, NHS). This guide supports tracking and informed clinician conversations and is not medical advice or diagnosis.
Routine Playbook
Turn scattered checking into a weekly routine you can sustain
This guide is built around repeatability: one capture rhythm, one monthly review habit, and one clearer way to see whether your process is working.
Best for readers who need a calm starting point before they change too many variables.
What this guide helps you decide
Understand hair miniaturization, identify it at home, and begin tracking before permanent follicle loss
Read this first if you want one clearer answer instead of another loop of broad browsing.
Best fit for this stage
Best for readers who need a calm starting point before they change too many variables.
Stay oriented while you read
Use this reading map to jump straight to the section you need now, or follow it top to bottom if you want the full logic.
Jump to sections
Most people think hair loss starts with hairs falling out. It does not. It starts with hairs getting thinner. The biological process behind pattern baldness is not sudden shedding but a slow, cycle-by-cycle shrinking of the hair follicle itself. This process is called miniaturization, and it is the single most reliable early indicator that androgenetic alopecia is underway. By the time you notice your hair looks thinner in photos or your scalp shows through under bright lights, miniaturization has likely been progressing for years. Understanding what it is, why it happens, and how to spot it gives you a real window of opportunity to act before the damage becomes permanent.
Track miniaturization before it becomes visible thinning
BaldingAI scores your hair density, thickness, and coverage from photos taken at home. Catch the earliest changes each month and build a timeline your dermatologist can actually use.
Use the BaldingAI hair tracking app to save one baseline session now, compare monthly checkpoints later, and keep one clear record for your next treatment or dermatologist decision.
What is hair miniaturization?
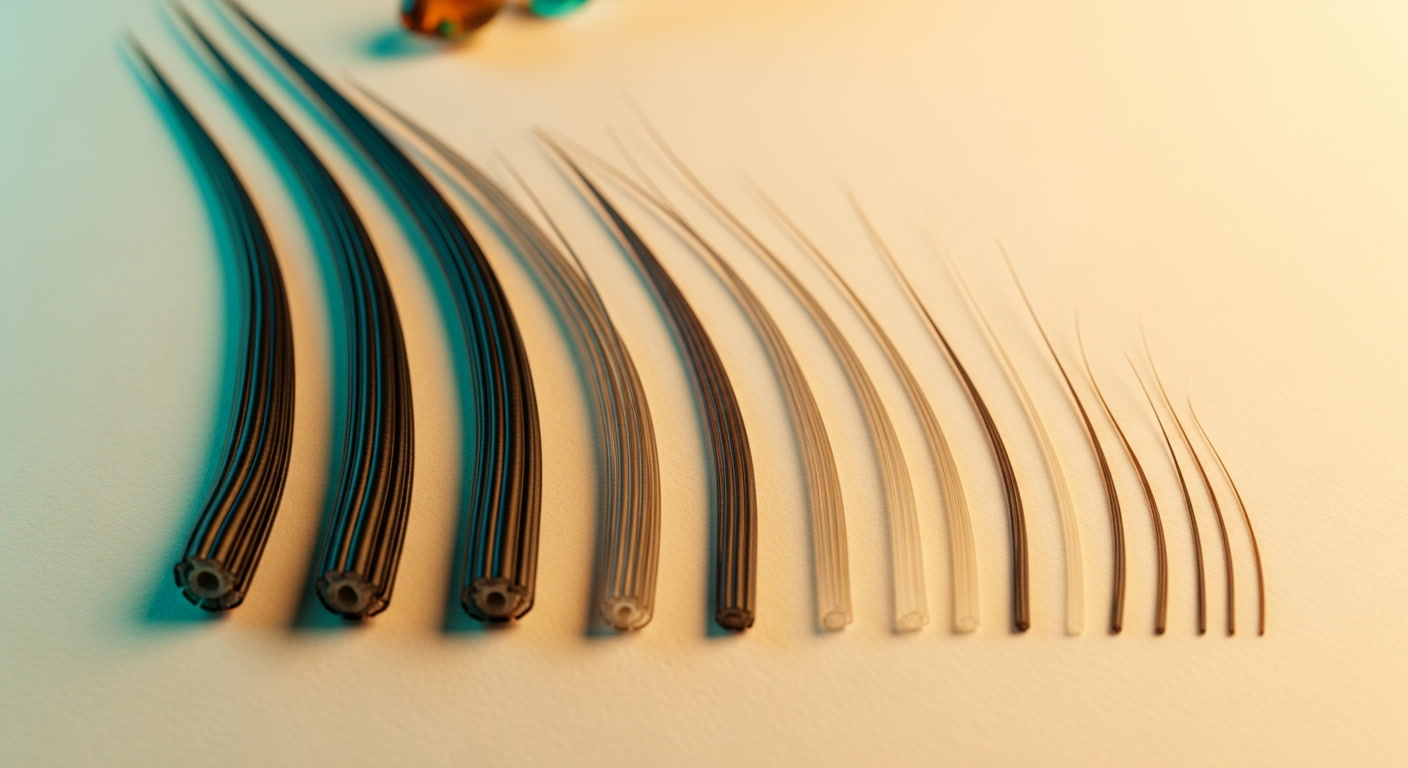
Hair miniaturization is the progressive shrinking of the hair follicle that causes each successive hair cycle to produce a thinner, shorter, and lighter strand. A healthy terminal hair is thick, pigmented, and grows for two to six years during the anagen (growth) phase. A miniaturized hair, by contrast, is fine, often unpigmented, and may grow for only a few weeks or months before entering the resting phase and falling out.
The process does not happen overnight. It unfolds across multiple hair cycles, each lasting roughly three to five years. With every cycle, the follicle produces a slightly thinner version of its previous hair. A strand that was once 80 micrometers in diameter might drop to 60, then 40, then 20. At the final stage, the follicle produces only vellus hair: the near-invisible peach fuzz that covers most of the body. Eventually, even vellus production can cease, leaving the follicle dormant or permanently closed.
This is the hallmark of androgenetic alopecia (AGA), the condition responsible for roughly 95% of hair loss in men and the majority in women. Sinclair et al. (2011) demonstrated in the British Journal of Dermatology that the ratio of miniaturized to terminal hairs is the most reliable trichoscopic marker for diagnosing AGA, often detectable years before the patient or even the clinician notices visual thinning. It is not the number of hairs you lose that signals pattern baldness. It is the caliber of the hairs that remain.
The science of follicle shrinkage
The driver of miniaturization in pattern hair loss is dihydrotestosterone (DHT), a potent androgen converted from testosterone by the enzyme 5-alpha reductase. DHT circulates through the bloodstream and binds to androgen receptors in the dermal papilla, the signaling center at the base of the hair follicle. In genetically susceptible follicles, this binding triggers a cascade of changes that progressively reduce the follicle's size and output.
The primary mechanism is a shortening of the anagen phase. A follicle that once sustained a hair for four years might sustain it for only one year, then six months, then a few weeks. As the growth phase shrinks, so does the maximum length and thickness the hair can achieve. The follicle itself physically contracts. Its dermal papilla loses cells, the surrounding connective tissue sheath thins, and the matrix that produces the hair shaft diminishes. Whiting (2001) described this process in detail in the Journal of the American Academy of Dermatology, showing that miniaturization in male pattern hair loss follows a predictable pattern: the terminal-to-vellus hair ratio in a healthy scalp is greater than 7:1, meaning for every vellus hair, there are at least seven thick terminal hairs. In early AGA, that ratio drops to 4:1 or lower. Once it falls below 2:1, thinning is usually visible to the naked eye.
Critically, not all follicles on the scalp respond to DHT equally. Follicles in the occipital region (the back and sides of the head) are largely androgen-resistant, which is why pattern baldness creates the characteristic horseshoe shape. Follicles at the temples, frontal hairline, and crown are the most DHT-sensitive, and they miniaturize first. This is also why hair transplants work: follicles moved from the back of the head to the top retain their genetic resistance to DHT.
How to spot miniaturization at home
You do not need a trichoscope or a dermatologist visit to identify early signs of miniaturization. The key indicator is mixed hair calibers in a localized area. Pull your hair back or part it at the temples, crown, or along your natural part line and look closely under bright, direct light. What you are looking for is thick hairs growing next to noticeably thin, wispy hairs in the same small patch of scalp.
Healthy scalp areas have relatively uniform hair thickness. When miniaturization begins, you will see a mix: full-caliber terminal hairs alongside shorter, finer hairs that appear almost translucent. These thin hairs may be lighter in color than your normal hair, even if you have never dyed it. They are shorter because their growth phase has been truncated, and they are finer because the follicle producing them has shrunk.
The temples and crown are the first areas affected in men. Women typically see it first along the central part. If you part your hair down the middle and see a widening strip of scalp with many fine, short hairs flanking the part, that is classic miniaturization. Under harsh overhead light, miniaturized areas appear thinner even when the actual hair count has not dropped significantly. The hair is still there, but each strand covers less area and blocks less light. This is why people often say "I can see my scalp now" before they notice any increase in shedding.
Photo comparison is one of the most effective self-assessment tools. A single photo tells you little, but two photos of the same spot taken three to six months apart under the same lighting reveal changes that the mirror alone cannot. Look for: a higher proportion of thin, light hairs; wider spacing between hairs; and more visible scalp. Wet hair or freshly towel-dried hair exaggerates these differences and makes miniaturization easier to spot.
Miniaturization vs. normal hair variation
Not every thin hair on your head is a sign of pattern baldness. Hair naturally varies in thickness across the scalp. The hairs along the hairline and at the nape tend to be finer than those on top. Body hair and facial hair have entirely different caliber profiles than scalp hair. Finding a few thin hairs mixed in with thick ones is normal on any head.
The distinction is context and pattern. Miniaturization is defined by finding thin hairs in areas where your hair was previously uniformly thick, and finding them in the specific zones that DHT targets. If you notice thin, wispy hairs at your temples or crown but the back of your head remains uniform and dense, that asymmetry is a red flag. If the thin hairs are scattered randomly across your entire scalp with no concentration in the DHT-sensitive zones, it is more likely normal variation or diffuse telogen effluvium rather than pattern loss.
Age matters too. Some degree of hair caliber reduction occurs naturally with aging, independent of androgenetic alopecia. This is called senescent alopecia and typically presents as uniform, gradual thinning across the entire scalp after age 50 or 60, without the characteristic pattern of AGA. In your 20s, 30s, or 40s, patterned miniaturization concentrated at the temples, crown, or part line is almost always androgenetic in origin.
The miniaturization ratio: what dermatologists measure
When you visit a dermatologist for hair loss, one of the most informative tests they can perform is trichoscopy: a magnified examination of the scalp using a specialized dermatoscope. The primary metric they extract from this exam is the miniaturization ratio, which quantifies the proportion of miniaturized hairs relative to terminal hairs in a given area.
Rakowska et al. (2009) established trichoscopic criteria for androgenetic alopecia, finding that more than 20% miniaturized hairs in the frontal scalp is a strong diagnostic indicator for AGA. In practice, a dermatologist will typically compare two sites: the frontal or temporal area (DHT-sensitive) and the occipital area (DHT-resistant). If the frontal area shows significantly higher miniaturization than the occipital, the diagnosis is clear.
Some clinics go further with HairCheck or TrichoScan devices that measure hair mass index and hair density with digital precision. These tools can detect a 10-15% change in hair caliber, well below what the human eye can perceive. If your dermatologist has access to trichoscopy or digital hair analysis, request a baseline measurement. That number becomes a reference point for every follow-up visit and gives both you and your doctor an objective way to determine whether your hair is stable, improving with treatment, or continuing to thin.
Why tracking miniaturization early matters
The urgency around miniaturization detection comes down to a biological fact: treatments can reverse early miniaturization, but they cannot resurrect dead follicles. Once a follicle has been miniaturized through enough cycles, it undergoes fibrosis. The dermal papilla is replaced by scar tissue, and the follicle loses its ability to produce any hair at all. At that point, no amount of finasteride, minoxidil, or microneedling will bring it back. Only surgical transplantation can place a new follicle in that spot.
Finasteride works by blocking 5-alpha reductase, reducing scalp DHT levels by approximately 60-70%. When DHT pressure drops, follicles in the early and mid stages of miniaturization can partially recover. The anagen phase lengthens again, and the next hair produced is thicker than the last. This is why clinical studies consistently show that finasteride is more effective at maintaining existing hair than regrowing hair that has been lost for years. The follicles that respond best are those that are still active but shrinking. Once they are gone, finasteride has nothing to work with.
Minoxidil operates through a different mechanism, increasing blood flow to follicles and extending the anagen phase. It can stimulate thicker growth from miniaturizing follicles, but the same rule applies: the follicle must still be alive. Combining both treatments targets miniaturization from two angles, which is why dermatologists increasingly recommend early combination therapy rather than waiting to see if one drug alone is sufficient.
The window of opportunity narrows with each hair cycle. If a typical cycle lasts three to five years and miniaturization progresses with each one, you may have only two or three cycles between "early, treatable miniaturization" and "irreversible follicle loss." That translates to roughly 6 to 15 years. It sounds like a long time, but those years pass without warning signs unless you are actively looking. By the time hair loss is obvious to others, much of that window has already closed.
How to track miniaturization with photos
Consistent photo tracking is the closest thing to trichoscopy you can do at home. The goal is to capture the same areas of your scalp under the same conditions at regular intervals, then compare side by side for changes in hair caliber, density, and scalp visibility. Here is a practical protocol.
Choose three target zones. Capture your temples (both sides), crown (top-down), and natural part line. These are the areas where miniaturization appears first in the vast majority of cases. If you are a woman, prioritize the part line and frontal area. If you are a man, prioritize the temples and crown.
Standardize your conditions. Use the same lighting every time. Bright, direct overhead light is best for revealing scalp visibility. Natural daylight from a window works well. Avoid flash photography, which flattens contrast. Shoot from the same distance and angle each session. Wet or freshly towel-dried hair shows miniaturization more clearly than dry, styled hair because wet hair clumps together, exposing the spaces between strands.
Capture monthly at minimum. Hair grows roughly one centimeter per month, and miniaturization progresses across cycles, not days. Monthly photos give you enough data to detect trends without creating anxiety from session-to-session noise. Pull up your oldest photo next to your newest every three months for a clear signal.
Look for four specific changes. (1) An increasing proportion of thin, light, short hairs relative to thick terminal hairs in the same zone. (2) Wider spacing between individual hairs, creating more visible scalp. (3) A shift in how the area looks under harsh overhead light compared to your earlier photos. (4) The hairline or part line appearing less defined, with wispy, irregular edges replacing the clean border you once had.
The power of photo tracking is that it removes subjectivity. You are not relying on how your hair "feels" today or what you think you see in the mirror after a bad night of sleep. You are comparing objective images captured under controlled conditions. That data is what separates productive monitoring from anxious mirror-checking. It is also what makes your dermatologist appointment ten times more useful: walking in with a six-month photo timeline gives your doctor concrete evidence to work with rather than relying solely on a single in-office exam.
For a structured self-assessment of where you stand on the pattern baldness scale, see our Norwood scale self-assessment guide. When you are ready to start tracking, use the early signs tracking template to set up your first baseline.
Build your miniaturization timeline
BaldingAI captures your temples, crown, and part line with guided positioning and scores each zone monthly. Three months of data gives you the trend line that tells you whether to act or simply keep watching.
Use the BaldingAI hair tracking app to save one baseline session now, compare monthly checkpoints later, and keep one clear record for your next treatment or dermatologist decision.
Use This Guide Well
For fundamentals content, the strongest signal is process quality: repeatable photos, stable scorecards, and comparable checkpoint windows.
- Lock one baseline capture session before changing multiple variables.
- Use weekly capture and monthly review to avoid panic from daily noise.
- Choose one guide and run it for a full checkpoint cycle before judging outcomes.
Safety note
This article is for education and tracking guidance. It does not replace diagnosis or treatment advice from a licensed clinician.
- Use matched photo conditions whenever possible.
- Review monthly trends instead of reacting to one photo day.
- Escalate persistent uncertainty or symptoms to clinician care.
Questions and Source Notes
How do I know if I'm actually losing hair or just overthinking it?
The most reliable way to tell is consistent photo documentation over time. A single photo or mirror check is unreliable because lighting, angles, and anxiety distort perception. Take standardized photos weekly — same angle, same lighting, same distance — and compare them monthly. If you see a clear directional trend across 3+ months, that is real signal, not noise.
When should I see a dermatologist about hair loss?
See a board-certified dermatologist if you notice persistent shedding for more than 3 months, visible scalp through hair that was previously dense, a receding hairline that has moved noticeably in the past year, or sudden patchy loss. Early intervention gives you more options. Bring 3+ months of tracking photos to make the visit more productive.
What is the first thing I should do if I notice thinning?
Start a tracking baseline immediately — before changing anything. Take clear photos of your crown, hairline, temples, and a top-down part view. Record the date, your current routine, and any medications. This baseline becomes the reference point for every future comparison, whether you decide to treat or just monitor.
Start early while your baseline is still clear
BaldingAI helps you build one clean baseline and a calm first month of tracking, so your next decision is based on evidence instead of panic.
Keep Reading From Here
Continue with the next article or matching tracking route that keeps this guide actionable instead of sending you back into broad browsing.
Next editorial reads
Tracking Hair Loss After a Haircut: How to Keep Photos Comparable
Foundational Guide · awareness
Terminal-to-Vellus Hair Ratio: The Metric Trichoscopists Actually Measure
Foundational Guide · awareness
Hair Loss Genetics: Can You Actually Predict Balding?
Foundational Guide · awareness
How to Read Hair Miniaturization on Trichoscopy Photos at Home
Foundational Guide · awareness